空鼻症候群
空鼻症候群,簡稱空鼻症,(英語:Empty Nose Syndrome,縮寫:ENS),在耳鼻喉科學中指的是通過鼻甲切除術過度切除鼻甲(通常為下鼻甲)後所造成的鼻腔異常及一系列併發症。

患者的症狀主要有:感受不到氣流(鼻阻力過低及鼻黏膜受損)、鼻腔乾燥、嗅覺下降、頭疼、精神不濟、身體易疲勞、注意力不集中等,時間長了易誘發哮喘和肺纖維化等。[1][2][3]
有研究顯示,在接受下鼻甲破壞性手術後,20%的患者會患上空鼻症。而中國工程院院士、北京同仁醫院院長韓德民教授認為,這個數字有可能更高。[4]
空鼻症候群是一種醫源性疾病,完全是可以避免的。
主要症狀
空鼻症的兩大症狀為:
- 慢性鼻腔乾燥。這一般會導致慢性黏膜炎症及疼痛。慢性發炎可以引致部份黏膜萎縮,有些研究因此稱其為「繼發性萎縮性發鼻炎」。[5][6][7][8][9]至少一項大型研究指出,萎縮性鼻炎的症狀平均需要7.1年後才會出現。研究還建議醫生注意早期症狀,並對病患者處方每日自行沖洗和潤濕鼻腔。[10]
- 矛盾性鼻阻。患者會感到鼻塞,而由於失去鼻黏膜來回饋氣流的感覺,這還會伴隨持續且經常出現的窒息感。產生這一感覺的三叉神經的萎縮、黏膜的乾涸和化生以及鼻甲切除術後的異常氣流運動都可能導致這種症狀。中樞神經系統接收不到持續的呼吸感覺,就會產生窒息、呼吸困難的感覺。[11][12][13]
其他主要症狀還包括睡眠困難和長期疲倦。[14]因為這些慢性症狀,所以患者的生活品質會大大降低,並會難以專注、產生焦慮及憂鬱。[15]另外可能出現的併發症還包括哮喘和慢性阻塞性肺病。[16][17][18]
病因

鼻腔中的鼻甲有著增潤、調節溫度、過濾空氣、控制氣流和感應氣流等作用。氣流進入鼻腔後,會繞過鼻甲,其結構有效提高空氣與鼻黏膜的接觸面積。鼻甲的功用對鼻部健康極為重要。其結構呈流線體,在處理空氣的同時並不阻礙氣流。[19]
鼻甲能夠保護內鼻黏膜,幫助其休息及再生。正常的成年人鼻腔能夠在24小時內處理1萬升空氣,因此鼻黏膜需要有一定的休息期,才可保證呼吸道上皮的健康。這種間斷的休息期稱為鼻週期。每3至6小時,血液充盈半邊鼻,使其休息和再生;另外一邊則不被充盈,進行大部份的呼吸工作。在下鼻甲切除後,鼻週期無法使血液完全充盈受損的一邊,因此喪失自然再生的能力。[20]
人類的鼻子一般有三對鼻甲:下鼻甲、中鼻甲和上鼻甲。每一對鼻甲的大小和形狀都非常不同,有著各自保護的鼻腔空間。下鼻甲最大,幾乎佔據整個鼻腔下部,從前部一直延伸到接近鼻咽處。由於下鼻甲處理大部份被吸入的空氣,所以一旦被損壞,會對剩餘的黏膜有極大的影響。中鼻甲位於下鼻甲之上,大約在鼻腔中部。中鼻甲相對較小,含有嗅覺神經軸突,且保護鼻腔上部,特別是位於頂部的嗅覺神經束以及篩竇和前額竇部份。中鼻甲的損壞對溫度、濕度的調節影響不大,但可能會降低嗅覺並影響篩竇和前額竇的健康。上鼻甲最小,是保護嗅球的最後一道防線。
如果損失過多的鼻甲組織,被切除部位周圍剩餘的黏膜會逐漸發炎、變乾、化生,並最終萎縮。鼻子的四大功能將會受到損害:呼吸、防禦、嗅覺和產生音韻。這一過程可以持續若干年,使得早期診斷非常困難。患者一般在鼻甲切除術後不久就能感覺到空鼻症的症狀。[14]
診斷
空鼻症的先兆包括:患者感到用鼻子呼吸困難,並有強烈的窒息感、鼻腔乾燥感。這些徵兆只在鼻甲切除術之後出現,有時甚至在幾年後才出現。
患者的鼻腔空間異常大,部份鼻甲喪失。某些患者的鼻黏膜因化生而乾燥,其他患者則有呈紅色的慢性發炎黏膜。硬化情況各異。[21]由於乾燥和過強的氣流,剩餘的組織很有可能有過度萎縮的情況。
預測
有關空鼻症候群的長時間觀察和研究很少。因為鼻甲切除術後的繼發性病症,所以空鼻症多年來都沒有受到正確的判斷。比如,剩餘的黏膜組織(鼻中隔以及其餘的鼻甲)通常會極度萎縮,造成實際的阻塞。
由於缺乏長時間觀察,因此目前還沒有數據顯示多少百分比病患者的症狀會迅速或大幅度的好轉。該病症的症狀是由實際鼻組織缺失、損害所造成的,所以能夠自行痊癒的可能性不高。
Eugene Kern博士首次使用「空鼻症候群」這一名詞。他認為,缺乏了鼻甲的保護,剩餘的鼻黏膜會暴露在未經過濾、未經調節的空氣,從而隨時間持續消耗和損壞,空鼻症的症狀也會因此逐漸惡化。他表示,當鼻甲組織少於某個臨界點後,鼻黏膜就無法從每時每刻的消耗中再生。一項在美國進行的試驗在幾年的時間內觀測了242位進行了各種鼻甲切除術的病人,他們在手術後產生了萎縮性鼻炎。在用電腦斷層和直接觀察這些病人的異常鼻腔結構後,科學家將這種情況命名為「空鼻症候群」。研究強調病症大大降低了病人的生活質量,而且病情有隨時間惡化的趨勢。[10]這一研究符合19世紀末醫學界採納鼻甲切除術以來空鼻症患者群體的結論。然而一些長期研究卻沒有發現長期的負面影響。目前爭議仍在持續,但醫學界傾向於在進行切除術時儘量保留鼻甲組織。[22]
病患者可以在鼻腔表面塗上保護性凝膠或使用鹽水噴劑來補充損失了的水分,從而避免黏膜組織萎縮。不過,完全重建下鼻甲才是解決這一病症的最徹底的方法。
有近期報告表示有可能通過在黏膜下注入填充物來重建下鼻甲。報告中的病人人數很少,後續觀察的時段也比較短,但報告的結論是正面的。[14][23][24]2010年的一項研究指出,通過手術進一步對「空鼻」進行切除可以改善鼻內氣流,但無法改變鼻子調節溫度、濕度的能力。這些功能將無法逆轉。[13]另一項研究表示,一旦受破壞的鼻黏膜使纖毛細胞退化、損失,則連用手術閉合鼻孔也無法使纖毛細胞重新增長。[10]
目前的治療方法
非手術治療
非手術治療通過保持鼻內濕度,避免感染和刺激,以及保證充分的血液供應,可以保持並改善剩餘鼻黏膜的健康。
- 用複方薄荷腦滴鼻液或者替代物保持鼻腔的水分,能緩解一定程度的乾燥。
- 用生理鹽水進行鼻沖洗。
- 睡眠時使用加濕器。
- 可適當服用維生素B2。
- 多喝水。
- 如果有臭鼻症(萎縮性鼻炎)的情況,則在進行鼻沖洗時加入80毫克慶大黴素。
- 許多空鼻症患者(約50%)會感到疼痛或憂鬱,可服用相應的藥物。
- 避免劇烈運動,通過一些舒緩的鍛鍊來保持整體生理健康,避免身體繼續衰竭,進一步惡化。
手術治療
Surgical treatment involves narrowing back the over enlarged nasal cavity—either by bulking up the partially resected turbinates with biological implant material (in cases where at least 50% of the inferior turbinate remain from anterior to posterior) or by creating neo-turbinates through submucosal implantation between the submucosa and bone in key locations in the nasal cavity. Of course, in some cases a combined approach is the best choice. The main difficulty with implant surgery is to achieve a long lasting bulk that will not get absorbed over time. Sometimes a procedure has to be repeated several times to get a sustainable result. The most physiological location for an implant is the lateral wall of the nasal cavity, where the inferior turbinate used to project from. An easier location to implant is the septum, but it is less favorable as it is not the natural location of the turbinates and may over obstruct the airflow.
The underlying rationale of surgery is to restore the natural inner nasal geometrical contours of the nasal passages of air (the inferior, middle, and superior meatuses), as much as possible, to mitigate the airflow just enough to restore normal rates of inner nasal humidity and temperature that will allow the mucosa to recuperate and sense the airflow well enough. It is paramount to do so while trying to restore the normal aerodynamics of the airflow in the nose, otherwise nasal obstruction will occur.
Pre-surgical planning has a tremendous impact on the success of the procedure. The surgeon is advised to perform a cotton test prior to the implantation: the surgeon places saline soaked chunks of cotton wool at the pre-planned site of implantation to simulate the implant. By doing so, he restricts and normalizes the nasal airflow patterns. This restores nasal aerodynamics. By trying different locations in accordance to the patient's feedbacks regarding the quality of his breathing and other ENS symptoms, it is possible to pinpoint the exact placement for the implants and their estimated shape and size.
Turbinate tissue is unique and there are no potential donor sites in the body from which to harvest similar tissue. However, in the nose, form equals function. It is therefore possible to restore some function by restoring the natural contours and proportions of the nasal passages: It is possible to create an artificial look-alike structure of a turbinate in the nasal cavities, and thus to regain some of the nose's capabilities to adequately resist, streamline, heat, humidify, filter, and sense the airflow.[14]
- A video demonstrating lateral wall implantation to create a bulk of tissue that will simulate the shape and function of the resected inferior turbinate. (頁面存檔備份,存於網際網路檔案館)
Implant materials

The bulking up of the sub-mucosa and mucosa to create a neo-turbinate structure can be achieved through implanting some supporting material between the bone/cartilage and also into the submucosal layer. Many materials have been tried over the past 100 years. In most cases this operation was used to restore heat and humidity to atrophic noses.
Generally speaking, the implant materials can be divided into 3 groups:
- autografts: bone, cartilage, fat, etc. from one site to another in the same patient. The problems here are relative shortage of tissue, and long term studies have shown high absorption rates in the nose. A Chinese study reported long-term success using iliac bone autografts.[25]
- foreign materials: such as fibrin glue, Teflon, Gore-Tex, and plastipore, which solve the problem of shortage of autografts, are easy to shape and do not tend to get absorbed. However they have a high extrusion rate, and sometimes cause infection. A case study of good retention of hydroxyapatite cement in one patient has been reported in 2000, but the follow-up was only 1 year long.[26]
- allografts: In the last two decades scientists have been able to harvest and remove away genetic markers of some basic human tissues (like skin dermis) from donors, and thus supplying a human natural implant material which does not stimulate the immune system to reject it. A good example for such material is acellular dermis (brand named "Alloderm"). It does not get rejected and in most areas retains most of its volume over long periods.[14]
The ideal implant material, other than real original turbinate tissue should be something with low extrusion and rejection rates, minimal infection risk, and—very importantly—that will provide a strong and endurable enough structure and at the same time allow good permeability for blood vessel incorporation, which seems to be the key against long term absorption.
其他圖像
-
 下鼻甲移除術後產生的空鼻症
下鼻甲移除術後產生的空鼻症 -
 移除所有鼻甲後的右側壁圖
移除所有鼻甲後的右側壁圖 -
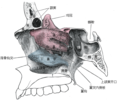 鼻腔解剖結構圖
鼻腔解剖結構圖



參考文獻
- ^ 王永臻. 下鼻甲部分切除术后并发空鼻综合征16例报告. 臨床耳鼻咽喉科雜誌. 2003, 17 (9).
- ^ 趙家利; 高春生; 張紅偉; 李爍. 空鼻综合征25例临床特征分析和诊治体会. 實用醫學雜誌. 2008, 24 (16).
- ^ 田興德; 塗德根; 孔維佳. 空鼻综合征. 臨床耳鼻咽喉頭頸外科雜誌. 2011, 25 (11).
- ^ 呼吸之痛_核心报道_新京报电子报. epaper.bjnews.com.cn. [2017-05-16].
- ^ Cottle MH. Nasal Atrophy, Atrophic Rhinitis, Ozena: Medical and Surgical Treatment. Journal Of The International College Of Surgeons. Volume 29(4), pages 472-484, 1958.
- ^ Passàli D, Lauriello M, Anselmi M, et al. Treatment of the inferior turbinate: long-term results of 382 patients randomly assigned to therapy. Ann Otol Rhinol Laryngol. 1999;108:569-75.
- ^ Moore GF, Freeman TJ, Yonkers AJ, Ogren FP. Extended follow-up of total inferior turbinate resection for relief of chronic nasal obstruction. by in Laryngoscope, volume 95, September 1985.
- ^ Berenholz L, et al'. Chronic Sinusitis: A sequela of Inferior Turbinectomy. American Journal of Rhinology, July–August 1998, volume 12, number 4.
- ^ Wang Y, Liu T, Qu Y, Dong Z, Yang Z. Empty nose syndrome. Zhonghua Er Bi Yan Hou Ke Za Zhi. 2001 Jun;36(3):203-5.
- ^ 10.0 10.1 10.2 Moore EJ & Kern EB. Atrophic rhinitis: A review of 242 cases. American Journal of Rhinology, 15(6), 2001.
- ^ Clarke RW, Jones AS, Charters P, et al. The role of mucosal receptors in the nasal sensation of airflow. Clin Otolaryngol. 1992;17:383-87.
- ^ Chhabra N. and Houser SM. The diagnosis and management of empty nose syndrome. Otolaryngologic Clinics of north America. 2009 (April);42(2):311-330,ix.
- ^ 13.0 13.1 Scheithauer MO. Surgery of the turbinates and 「empty nose」 syndrome. GMS Current Topics in Otorhinolaryngology – Head and Neck Surgery 2010. Vol 9:Doc03. doi: 10.3205/cto000067 (頁面存檔備份,存於網際網路檔案館)
- ^ 14.0 14.1 14.2 14.3 14.4 Houser SM. Surgical Treatment for Empty Nose Syndrome. Archives of Otolaryngology Head & Neck Surgery\ Vol 133 (No.9) Sep' 2007: 858-863.
- ^ Rice DH, Kern EB, Marple BF, Mabry RL, Friedman WH. The turbinates in nasal and sinus surgery: a consensus statement. Ear Nose Throat J. 2003;82(2):82-84.
- ^ Bionity Life Science Encyclopedia on empty nose syndrome.
- ^ Hens G, Hellings PW. The nose: gatekeeper and trigger of bronchial disease, Rhinology 2006 Sep; 44(3):179-87.
- ^ Hellings PW, Prokopakis EP. Global airway disease beyond allergy, Curr Allergy Asthma Rep. 2010 Mar;10(2):143-9.
- ^ Wolf M, Naftali S, Schroter RC, Elad D. Air-conditioning characteristics of the human nose. The Journal of Laryngology & Otology February 2004, Vol. 118, pp. 87–92.
- ^ Hasegawa M, Kern EB. The human nasal cycle. Mayo Clin Proc. 1977 Jan;52(1):28-34.
- ^ Huizing & de-Groot. Functional Reconstructive Nasal Surgery. Thieme. 2003: 64–65. ISBN 1-58890-081-9.
- ^ Hol MKS. & Huizing EH. Treatment of inferior turbinate pathology: a review and critical evaluation of the different techniques. Rhinology, 38, 157-166, 2000.
- ^ Wang Y, Liu T, Qu Y, Dong Z, Yang Z. Empty Nose Synrome. Zhonghua Er Bi Yan Hou Ke Za Zhi. 2001 Jun;36(3):203-5. Chinese.
- ^ Rice DH. Rebuilding the inferior turbinate with hydroxyapatite cement. Ear Nose Throat J. 2000 Apr;79(4):276-7.
- ^ Wang Y, Liu T, Qu Y, et al. [Empty nose syndrome]. Zhonghua Er Bi Yan Hou Ke Za Zhi 2001;36(3):203–5 [Chinese].
- ^ Rice DH. Rebuilding the inferior turbinate with hydroxyapatite cement. Ear Nose Throat J 2000;79(4):276–7.
外部連結
- Empty Nose Syndrome Association (More symptoms, and a turbinates tutorial on life threatening risks in ENS)
- Dr. Houser's tutorial pages on ENS
- Internet support forum for ENS sufferers (頁面存檔備份,存於網際網路檔案館)
- "Sniffing At Empty Nose Idea" (Aaron Zitner, The Los Angeles Times, 2001) (頁面存檔備份,存於網際網路檔案館)
- Dr. Dondè's pages on ENS not surgical treatment by platelet grown factor